Información General Información General |
| Artículos |
| Notícias |
| Enlaces |
| Contactar |
| Buscar |
| Premio Nadal |
| Formación Continuada |
 |


INCISIONES PARA EXODONCIA DE TERCEROS MOLARES IMPACTADOS. REVISIÓN DE LA LITERATURA |
|
Publicado el: 30/12/2011 09:56:39  | |
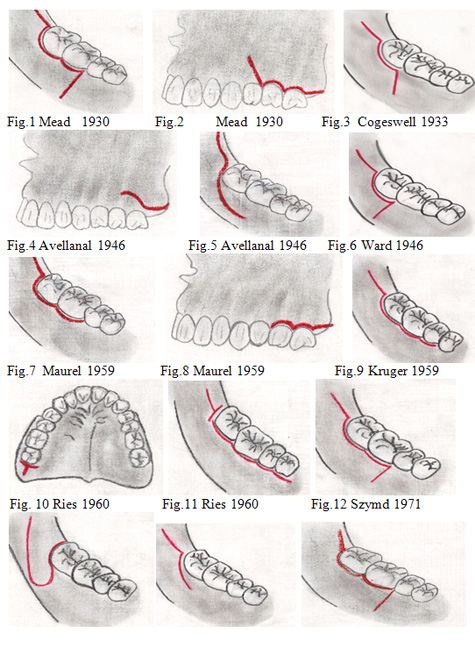
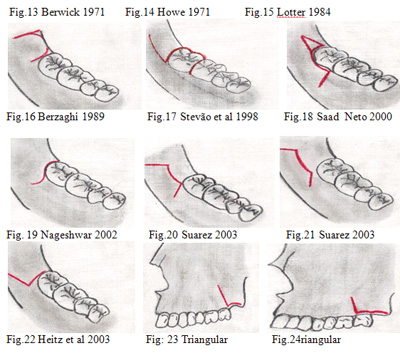
AUTORES Blanco GE, Odontólogo U Metropolitana, Clínica Codes, ȸ Giovanetti K, Odontóloga U de Campina, Clinica Unicamp Limeira, ǂGuerrero JS, Cirujano Oral Y Maxilofacial, U Javeriana, Práctica Privada. RESUMEN Los terceros molares pueden presentarse total y/o parcialmente impactados, estos pueden ser mucosos, submucosos, o completamente impactados en el hueso maxilar , la técnica quirúrgica incluye un tipo de incisión, esta desempeña un papel fundamental en la cicatrización, presentamos una serie de incisiones descritas por diferentes trabajos, es criterio de cada profesional emplearla de acuerdo a sus necesidades y conveniencias. ABSTRAC The total third molars can occur and / or partially impacted, they may be mucous, submucous, or completely impacted in the maxillary bone and jawbone, surgical technique includes an incision type, this plays a role in healing, we present a series of incisions described by different jobs, it is professional discretion of each employee according to their needs and interests. PALABRAS CLAVE Terceros molares, impactación, incisiones KEYS WORDS Third molar teeth, impacted, flap design INTRODUCCIÓN La cirugía de terceros molares impactados y/o parcialmente impactados es el procedimiento más común en la cirugía oral y maxilofacial1-18, sus indicaciones terapéuticas van desde; historia previa de infección19-22,enfermedad periodontal23-29, pericoronitís30-33, manejo de un dolor inexplicable34, dolor asociado al tercer molar35-36, caries no tratable, prevención de caries37-43, reabsorción de raíces de dientes adyacentes35,44-46, consideraciones ortodónticas, apiñamiento de incisivos inferiores47-52, consideraciones protésicas53, prevención y/o asociación con de fracturas mandibulares14,54-58, profilaxis45,61-65, consideraciones sistémicas de salud66-88, quistes y tumores13,61,90,91, interferencia en la cirugía ortognatica o su reconstrucción de la mandibula92, dientes para el uso de transplantes93, dientes involucrados dentro del campo de recesión de un tumor34,94 , dientes antagonistas que no cumplen ningún papel en la oclusión62,95. La controversia en el tratamiento de los terceros molares esta orientada por 2 corrientes filosóficas de profesionales, los intervencionistas que están a favor de la remoción profiláctica de los terceros molares impactados total y/o parcialmente sintomáticos y libre da alguna patología, amparados en las indicaciones para evitar una serie de complicaciones, sin embargo no hay evidencias científicas que afirmen o nieguen que todos estos procedimientos favorecen la salud del paciente91,97-99. Dentro de las complicaciones más frecuentes están; ansiedad pre y pos quirúrgica 100-101, dolor, trismus, infección, alvéolo seco102-107, como una medida para prevenir estos riesgos y complicaciones se ha propuesto que la técnica quirúrgica y la experiencia del cirujano son esenciales para el manejo adecuado de eventuales complicaciones1,35. Dentro de La técnica quirúrgica incluye; diseño de colgajo, técnica de remoción ósea, método de seccionamiento del diente, colocación de drenajes, exposición intencional del alvéolo y técnica de sutura108, trataremos la incisión, muchos autores han propuesto diferentes incisiones109-123 Fig 1-24, cada una de estas ha sido propuesta para lograr un acceso adecuado y disminuir los efectos secundarios del procedimiento como son; dolor, trismus, inflamación, alvéolo seco e infección, reducir las complicaciones ha sido el propósito de los planteamientos de muchos estudios sobre el uso de estas incisiones. Otra gran preocupación son los defectos periodontales que podrían surgir en la superficie distal al 2 molar después de la remoción de terceros molares impactados, se han reportado publicaciones de frecuencia de alteraciones periodontales , relacionados con la edad, inclinación del molar, placa visible en la superficie distal al 2 molar124. Pero estos problemas periodontales presentan resultados contradictorios de acuerdo a los estudios reportados, mientras unos reportan una disminución de la altura ósea distal al 2 molar, después de la extracción del molar impactado, otros manifiestan que se incremento la altura después de la cirugía, esta altura puede verse afectada con el sólo hecho de levantar un colgajo sin osteotomía125. Para Nageshwar, La incisión no debe realizarse sobre defectos óseos, ni cortar el musculo o tendón, estas incisiones no deben ser muy extensa, estas podrían influenciar en las consecuencias desafortunadas de la extracción 123. El diseño de colgajo según Karaca et al125,usado durante la cirugía de remoción de terceros molares impactados previene complicaciones relacionadas con el estado periodontal del 2 molar. Súarez et al consideran que este diseño tiene influencia en la cicatrización primaria122, esta evita la dehiscencia de la herida y se ha evaluado la técnica de sutura para lograr este cierre124, para Sanchis et al opinan que el cierre primario evita el drenaje del alvéolo y empeora el postoperatorio de inflamación y dolor, optan por colocar drenes, obteniendo un postoperatorio menos doloroso127. El colgajo envolvente según Kirk et al, presenta una incidencia de dehiscencias de la herida, lo que podría inducir a un alveolo seco y un periodo post-operatorio doloroso e incomodo128 , daño a nivel de las fibras de inserción periodontales a nivel cervical cuando se realiza la incisión, el colgajo triangular presenta un índice de inflamación mayor y mejor visibilidad operatoria128. Sandhu et al reportan en su estudio de comparación de dos tipos de colgajos, el colgajo envolvente presento mayor inflamación y dehiscencia que el colgajo tipo bayoneta (Triangular) usado para comparar los efectos de dolor, inflamación, trismus, dehiscencia de la herida después de la exodoncia de terceros molares impactados, el grado de inflamación según diversos autores está influenciado por el grado de erupción (Parcial o Total) y la angulación, para ellos no hubo diferencias y hubo una incidencia de inflamación muy baja de molares verticales comparadas con los mesio-angulares, el grado de inflamación no estuvo relacionado con la duración de la cirugía129. Para Arta et al, el tipo de incisión no tiene efectos sobre la salud periodontal distal al segundo molar, pero podría influenciar en la cicatrización primaria de la herida y un grado de osteítis alveolar130. Martins et al, realizaron una comparación de 2 tipos de colgajos ( Semejantes al Avellanal y Marzola) y no encontraron diferencias significativas referentes a la cicatrización periodontal al segundo molar y consideran que deben analizarse otros factores como son; edad del paciente, superficie de contacto entre 2 y 3 molar, tamaño del folículo pericoronario, presencia de inflamación periodontal pre-existente, tipo de retención, cantidad de hueso removido, cantidad de encia adherida distal al 2 molar, proximidad con la rama ascendente de la mandíbula y tipo de sutura y habilidad del profesional131. Erdogan et al, comparan 2 tipos de colgajo (Envolvente y Triangular) y el primero presenta menor grado de inflamación que el segundo, no hay diferencia significativa en el grado de trismus entre los dos colgajos, tiempo operatorio, número de analgésicos tomados, recomiendan el colgajo envolvente por presentar menor índice de inflamación108. Kırtıloğlu et al, comparan 2 tipos de colgajo (Szmyd y Triangular o Paramarginal) no encontraron diferencia en la cicatrización, recomiendan una extracción quirúrgica con mínimo trauma y el colgajo de Szmyd presenta una encía intacta distal al segundo molar y una cicatrización periodontal comparado con el otro colgajo después de la extracción de molares impactados completamente en posición horizontal o mesioangular. Jakse et al, concluyen que el colgajo envolvente produce más dehiscencias que el colgajo de Szmyd y esto repercute en la cicatrización primaria, esto produce un periodo postoperatorio más largo, doloroso e incomodo para el paciente. Pascualini et al, reportan que el cierre secundario después de la exodoncia de terceros molares impactados, ofrece resultados considerando las variables de dolor e inflamación, reduciendo la incomodidad en el postoperatorio y que el cierre primario pude ser más doloroso y producir una osteítis alveolar. DISCUSIÓN Existe una variedad de propuestas de incisiones para el abordaje de terceros molares impactados, pero no son claras las conclusiones de esos trabajos y tienden a ser controversiales, muchos trabajos carecen de un número reducido de casos y las variables que se investigan podrían ser excluyentes, se habla mucho de la experiencia del cirujano para evitar las complicaciones, del tiempo operatorio, sin embargo todos los procedimientos siempre reportan complicaciones como; trismus, dolor, inflamación, dificultad en la apertura bucal, y otras no se tienen en cuenta como los factores de calidad de vida del paciente, afectada notablemente. CONCLUSIONES 1- Los colgajos no presentan alteraciones a nivel periodontal distal al segundo molar 6 meses después de la exodoncia, por lo tanto el diseño de colgajo es una problema de preferencia individual del cirujano, y del tipo de entrenamiento recibido108,123,126,127,128, 130, ,135,136, muchas técnicas requieren un entrenamiento previo para manejarlas adecuadanmente123. 2-Si hay un problema relacionado con los tejidos blandos alrededor de los segundos molares mandibulares, es aparentemente no es un resultado de la cirugía o la técnica, pero es la resultado de otro proceso. Otros estudios comparativos Aún se necesitan para determinar la mejor técnica125. 3- El tipo de colgajo no disminuye los efectos como; inflamación, dolor y mejor apertura bucal después de la extracción, la ausencia de incremento en la profundidad no está relacionada con el tipo de colgajo usado, es el resultado de una técnica conservadora122-136 . 4- Los pocos estudios que realizan una comparación entre las diferentes técnicas de incisión no encuentran una diferencia significativa sobre los efectos adversos de la cirugía de terceros molares con respecto a; perdida de unión periodontal, índice de placa, nivel óseo distal al segundo molar, margen gingival, profundidad del sondeo periodontal, inflamación, dolor, trismus, apertura bucal, no presentan diferencias significativas que puedan demostrar que una incisión debe ser usada con preferencia122-136 sobre otra para mejorar la calidad de vida del paciente
BIBIOGRAFIA
1- Bouloux G, Steed M, Perciaccante V. Complications of Third Molar Surgery. Oral Maxillofacial Surg Clin N Am 2007; 19: 117-128. 2- Amarillas E, Toranzo J, Martínez R, Loyola M, Hidalgo J, Fierro V, Gordillo A, Pozos A. Use of Therapeutic Laser After Surgical Removal of Impacted Lower Third Molars. J Oral Maxillofac Surg. 2010;68:319-324. 3- Farish S, Bouloux G. General Technique of Third Molar Renoval. Oral Maxillofacial Surg Clin N Am 2000; 19: 23-43. 4- Susarla S, Dodson T. Preoperative Computed Tomography Imaging in the Management of Impacted Mandibular Third Molars. J Oral Maxillofac Surg2007; 65:83-88.
5- Graziani F, D'Aiuto F,Arduino P, Tonelli M, Gabriele M. Perioperative dexamethasone reduces post-surgical sequelae of wisdom tooth removal. A splitmouth randomized double-masked clinical trial. Int. J. Oral Maxillofac. Surg. 2006;35: 241-246. 6- Adeyemo WL, James O, Ogunlewe MO, Ladeinde AL, Taiwo OA, Olojede AC. Indications for extraction of third molars: a review of 1763 cases. Niger Postgrad Med J. 2008;15(1):42-46. 7- Susarla S, Blaese Br, Magalnick D. Third molar surgery and associated complications. Oral Maxillofacial Surg Clin N Am 2003;15:177-186. 8- Pozos A, Martínez R, Aguirre P, Pérez J. Tramadol Administered in a Combination of Routes for Reducing Pain After Removal of an Impacted Mandibular Third Molar. J Oral Maxillofac Surg, 2007;65: 1633-1639. 9-Kirmeier R, Truschnegg A, Payer M, Acham S, Schulz K, Jakse N. Evaluation of a muscle relaxant on sequelae of third molarsurgery: a pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 104: e8-e14. 10- Blondeau F,Daniel N. Extraction of Impacted Mandibular Third Molars: Postoperative Complications and Their Risk Factors. Jcda 2007; 73(4):325
11-Abu-El Naaj I, Braun R, Leiser Y, Peled M. Surgical Approach to Impacted Mandibular Third Molars-Operative Classification. J Oral Maxillofac Surg 2010; 68:628-633. 12- Guillaume B, Lacoste JP, Gaborit N, Brossard G, Cruard A, Basl´e MF, Chappard D. Microcomputed tomography used in the analysis of the morphology of root canals in extracted wisdom teeth. British Journal of Oral and Maxillofacial Surgery 2006; 44: 240-244.
13- Adeyemo WL. Do pathologies associated with impacted lower third molars justify prophylactic removal? A critical review of the literatura. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 102:448-52. 14- Wagner KW, Otten JE, Schoen R . Schmelzeisen R.: Pathological mandibular fractures following third molar removal. Int. J. Oral Maxillofac. Surg. 2005; 34: 722-726. 15- Lübbers HT, Matthews F, Damerau G, Kruse AL, Obwegeser JA, Grätz KW, Eyrich GK. Anatomy of impacted lower third molars evaluated by computerized tomography: is there an indication for 3-dimensional imaging? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011; 111:547-550. 16- Kunkel M, Doz P, Morbach T, Kleis W, Wagner W. Third molar complications requiring hospitalization. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 102:300-306. 17-Kim HR, Choi BH, Engelke W, Serrano D, Xuan F, Mo DY. A comparative study on the extractions of partially impacted mandibular third molars with or without a buccal flap: a prospective study. J Oral Maxillofac Surg. 2011; 69(4):966-970. 18-Offenbacher S, Lieff S, Boggess KA, et al. Maternal periodontitis and prematurity. Part I: Obstetric outcome of prematurity and growth restriction. Ann Periodontol 2001; 6:164-174. 19- White RP Jr, Madianos PN, Offenbacher S, Phillips C, Blakey GH, Haug RH, Marciani RD. Microbial complexes detected in the second/third molar region in patients with asymptomatic third molars. J Oral Maxillofac Surg. 2002; 60(11):1234-1240. 20- Flynn TR, Shanti RM, Levi MH, Adamo AK, Kraut RA, Trieger N.Severe odontogenic infections, part 1: prospective report.J Oral Maxillofac Surg. 2006; 64(7):1093-1103. 21- Flynn TR, Shanti RM, Hayes C.Severe odontogenic infections, part 2: prospective outcomes study. J Oral Maxillofac Surg. 2006; 64(7):1104-1113. 22- Sánchez AR, Kupp LI, Sheridan PJ, Sánchez DR.Maternal chronic infection as a risk factor in preterm low birth weight infants: the link with periodontal infection. J Int Acad Periodontol. 2004; 6(3):89-94. 23- Blakey GH, Marciani RD, Haug RH, Phillips C, Offenbacher S, Pabla T, White RP Jr. Periodontal pathology associated with asymptomatic third molars. J Oral Maxillofac Surg. 2002; 60(11):1227-1233. 24- White RP Jr, Offenbacher S, Phillips C, Haug RH, Blakey GH, Marciani RD. Inflammatory mediators and periodontitis in patients with asymptomatic third molars.J Oral Maxillofac Surg. 2002; 60(11):1241- 1245. 25- White RP Jr, Offenbacher S, Blakey GH, Haug RH, Jacks MT, Nance PE, Phillips C. Chronic oral inflammation and the progression of periodontal pathology in the third molar region.J Oral Maxillofac Surg. 2006; 64(6):880-885. 26- Blakey GH, Jacks MT, Offenbacher S, Nance PE, Phillips C, Haug RH, White RP Jr. Progression of periodontal disease in the second/third molar region in subjects with asymptomatic third molars. J Oral Maxillofac Surg. 2006; 64(2):189-193. 27-Blakey GH, Parker DW, Hull DJ, White RP Jr, Offenbacher S, Phillips C, Haug RH. Impact of removal of asymptomatic third molars on periodontal pathology.J Oral Maxillofac Surg. 2009; 67(2):245-250. 28- Rajasuo A, Sihvonen OJ, Peltola M, Meurman JH.Periodontal pathogens in erupting third molars of periodontally healthy subjects. Int J Oral Maxillofac Surg. 2007; 36(9):818-821. 29- White RP Jr, Phillips C, Hull DJ, Offenbacher S, Blakey GH, Haug RH. Risk markers for periodontal pathology over time in the third molar and non-third molar regions in young adults. Int J Oral Maxillofac Surg. 2008; 66(4):749-754. 30- Peltroche H, Reichhart E, Schmitt W, Lütticken R, Haase G. Investigation of infectious organisms causing pericoronitis of the mandibular third molar. J Oral Maxillofac Surg. 2000; 58(6):611-616. 31-Sixou JL, Magaud C, Jolivet-Gougeon A, Cormier M, Bonnaure-Mallet M. Evaluation of the mandibular third molar pericoronitis flora and its susceptibility to different antibiotics prescribed in france. J Clin Microbiol. 2003; 41(12):5794-5797. 32-Fuster MA, Gargallo J, Berini L, Gay- C. Evaluation of the indication for surgical extraction of third molars according to the oral surgeon and the primary care dentist. Experience in the Master of Oral Surgery and Implantology at Barcelona University Dental School. Med Oral Patol Oral Cir Bucal. 2008; 13(8):E499-504. 33- Mohammed-Ali RI, Collyer J, Garg M. Osteomyelitis of the mandible secondary to pericoronitis of an impacted third molar. Dent Update. 2010; 37(2):106-108. 34-Marciani RD. Third Molar Removal: An Overview of Indications, Imaging, Evaluation, and Assessment of Risk. Oral Maxillofacial Surg Clin N Am 2007; 19;1-13. 35-Kaushik SK, Gupta SK. Impacted Third Molar Surgery and the Aviator. Ind J Aerospace Med 2010; 54(1): 26-31. 36-Chaparro A, Pérez S, Valmaseda E, Berini L, Gay C. Morbidity of third molar extraction in patients between 12 and 18 years of age.Med Oral Patol Oral Cir Bucal 2005; 10:422-431. 37- Ahmad N, Gelesko S, Shugars D, White RP Jr, Blakey G, Haug RH, Offenbacher S, Phillips C.Caries experience and periodontal pathology in erupting third molars. J Oral Maxillofac Surg. 2008; 66(5):948-953. 38- Garaas R, Moss KL, Fisher EL, Wilson G, Offenbacher S, Beck JD, White RP Jr. Prevalence of visible third molars with caries experience or periodontal pathology in middle-aged and older Americans.J Oral Maxillofac Surg. 2011; 69(2):463-470. 39- Fisher EL, Moss KL, Offenbacher S, Beck JD, White RP Jr.Third molar caries experience in middle-aged and older Americans: a prevalence study. J Oral Maxillofac Surg. 2010; 68(3):634-640. 40- Ozeç I, Hergüner Siso S, Taşdemir U, Ezirganli S, Göktolga G. Prevalence and factors affecting the formation of second molar distal caries in a Turkish population. Int J Oral Maxillofac Surg. 2009; 38(12):1279-1282. 41- Chang SW, Shin SY, Kum KY, Hong J. Correlation study between distal caries in the mandibular second molar and the eruption status of the mandibular third molar in the Korean population.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108(6):838-843. 42- McArdle LW, Renton TF.Distal cervical caries in the mandibular second molar: an indication for the prophylactic removal of the third molar? Br J Oral Maxillofac Surg. 2006; 44(1):42-45. 43- Shugars DA, Elter JR, Jacks MT, White RP, Phillips C, Haug RH, Blakey GH. Incidence of occlusal dental caries in asymptomatic third molars. J Oral Maxillofac Surg. 2005; 63(3):341-346. 44- Allen RT, Witherow H, Collyer J, Roper-Hall R, Nazir MA, Mathew G. The mesioangular third molar--to extract or not to extract? Analysis of 776 consecutive third molars. Br Dent J. 2009 Jun 13;206(11):E23; discussion 586-587. 45- Minoru Yamaoka M, Furusawa K, Ikeda M, Hasegawa T. Root resorption of mandibular second molar teeth associated with the presence of the third molars. Australian Dental Journal 1999; 44:(2):112-116. 46-Nitzan D. Keren T. Marmary Y. Does an impacted tooth cause root resoption of the adjacent one? Oral Surg. 1981; 51: 221-224. 47- Bagheri S, Ali Khan H. Extraction Versus Nonextraction Management of Third Molars. Oral Maxillofacial Surg Clin N Am 2007;19:15-21. 48- Sidlauskas A, Trakiniene G.Effect of the lower third molars on the lower dental arch crowding. Stomatologija. 2006; 8(3):80-84. 49- Bernabé E, Flores C. Dental morphology and crowding. A multivariate approach. Angle Orthod. 2006; 76(1):20-25. 50- Niedzielska I.Third molar influence on dental arch crowding. Eur J Orthod. 2005; 27(5):518-523. 51- Harradine NW, Pearson MH, Toth B. The effect of extraction of third molars on late lower incisor crowding: a randomized controlled trial. Br J Orthod. 1998 ; 25(2):117-122. 52- Al-Balkhi KM.The effect of different lower third molar conditions on the re-crowding of lower anterior teeth in the absence of tight interproximal contacts one-year post orthodontic treatment: a pilot study. J Contemp Dent Pract. 2004; 15;5(3):66-73. 53-Nance PE, White RP Jr, Offenbacher S, Phillips C, Blakey GH, Haug RH.Change in third molar angulation and position in young adults and follow-up periodontal pathology.J Oral Maxillofac Surg. 2006; 64(3):424-428. 54- Grau V, Gargallo J, Almendros N, Gay C. Mandibular fractures related to the surgical extraction of impacted lower third molars: a report of 11 cases.J Oral Maxillofac Surg. 2011; 69(5):1286-1290. 55- Al-Belasy FA, Tozoglu S, Ertas U. Mastication and late mandibular fracture after surgery of impacted third molars associated with no gross pathology. J Oral Maxillofac Surg. 2009; 67(4):856-861. 56- Chrcanovic BR, Custódio AL. Considerations of mandibular angle fractures during and after surgery for removal of third molars: a review of the literature. J Oral Maxillofac Surg. 2010; 14(2):71-80. 57- Libersa P, Roze D, Cachart T, Libersa JC. Immediate and late mandibular fractures after third molar removal. J Oral Maxillofac Surg. 2002; 60(2):163-5; discussion 165-166. 58- Marquez IM, Stella JP. Modification of sagittal split ramus osteotomy to avoid unfavorable fracture around impacted third molars. Int J Adult Orthodon Orthognath Surg. 1998; 13(3):183-187. 59- Santos S, Moreira R, Araújo M. Treatment of a Mandibular Angle Fracture by Champy's Method after Removal of Contralateral Impacted Third Molar: Case Report. Rev. Cir. Traumatol. Buco-Maxilo-fac., Camaragibe. 2009; 9(3):15-20. 60-Bodner L, Brennan PA, McLeod NM. Characteristics of iatrogenic mandibular fractures associated with tooth removal: review and analysis of 189 cases. Br J Oral Maxillofac Surg. 2011; 49(7):567-572. 61- Stathopoulos P, Mezitis M, Kappatos C, Titsinides S, Stylogianni E. Cysts and tumors associated with impacted third molars: is prophylactic removal justified? J Oral Maxillofac Surg. 2011; 69(2):405-408. 62- Jasinevicius TR, Pyle MA, Kohrs KJ, Majors JD, Wanosky LA. Prophylactic third molar extractions: US dental school departments' recommendations from 1998/99 to 2004/05. Quintessence Int. 2008; 39(2):165-176. 63- Adeyemo WL. Do pathologies associated with impacted lower third molars justify prophylactic removal? A critical review of the literature.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102(4):448-452. 64- Almendros N, Alaejos E, Quinteros M, Berini L, Gay C. Factors influencing the prophylactic removal of asymptomatic impacted lower third molars.Int J Oral Maxillofac Surg. 2008; 37(1):29-35. 65-Anderson M. Removal of asymptomatic third molars: indications, contraindications, risks and benefits.J Indiana Dent Assoc. 1998; 77(1):41-46. 66- Song F, O'Meara S, Wilson P, Golder S, Kleijnen J.The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth. Semin Orthod. 1999; 5(3):191-204. 67-Song F, Landes DP, Glenny AM, Sheldon TA.Prophylactic removal of impacted third molars: an assessment of published reviews. Br Dent J. 1997; 182(9):339-346. 68- Matevosyan NR. Periodontal disease and perinatal outcomes. Arch Gynecol Obstet. 2011; 283(4):675-686. 69- Khader Y, Al-shishani L, Obeidat B, Khassawneh M, Burgan S, Amarin ZO, Alomari M, Alkafajei A.Maternal periodontal status and preterm low birth weight delivery: a case-control study. Arch Gynecol Obstet. 2009; 279(2):165-169. 70- Sacco G, Carmagnola D, Abati S, Luglio PF, Ottolenghi L, Villa A, Maida C, Campus G. Periodontal disease and preterm birth relationship: a review of the literature. Minerva Stomatol. 2008; 57(5):233-46, 246-250. 71- Pitiphat W, Joshipura KJ, Gillman MW, Williams PL, Douglass CW, Rich-Edwards JW. Maternal periodontitis and adverse pregnancy outcomes. Community Dent Oral Epidemiol. 2008; 36(1):3-11. 72- Siqueira FM, Cota LO, Costa JE, Haddad JP, Lana AM, Costa FO. Intrauterine growth restriction, low birth weight, and preterm birth: adverse pregnancy outcomes and their association with maternal periodontitis. J Periodontol. 2007; 78(12):2266-2276. 73- Toygar HU, Seydaoglu G, Kurklu S, Guzeldemir E, Arpak N. Periodontal health and adverse pregnancy outcome in 3,576 Turkish women. J Periodontol. 2007; 78(11):2081-2094. 74- Sharma R, Maimanuku LR, Morse Z, Pack AR. Preterm low birth weights associated with periodontal disease in the Fiji Islands. Int Dent J. 2007; 57(4):257-260. 75- Sánchez AR, Bagniewski S, Weaver AL, Vallejos N. Correlations between maternal periodontal conditions and preterm low birth weight infants. J Int Acad Periodontol. 2007; 9(2):34-41. 76- Madrid C, Bouferrache K, Pop S, Abarca M.-Is atherosclerosis a periodontally-induced disease?. Rev Med Suisse. 2009; 5(227):2388-2393. 77- Kshirsagar AV, Moss KL, Elter JR, Beck JD, Offenbacher S, Falk RJ. Periodontal disease is associated with renal insufficiency in the Atherosclerosis Risk In Communities (ARIC) study. Am J Kidney Dis. 2005; 45(4):650-657. 78- Craig RG, Spittle MA, Levin NW. Importance of periodontal disease in the kidney patient. Blood Purif. 2002; 20(1):113-119. 79- D'Aiuto F, Ready D, Tonetti MS. Periodontal disease and C-reactive protein-associated cardiovascular risk. J Periodontal Res. 2004; 39(4):236-241. 80- D'Aiuto F, Parkar M, Andreou G, Brett PM, Ready D, Tonetti MS. Periodontitis and atherogenesis: causal association or simple coincidence? J Clin Periodontol. 2004; 31(5):402-411. 81- Glurich I, Grossi S, Albini B, Ho A, Shah R, Zeid M, Baumann H, Genco RJ, De Nardin E. Systemic inflammation in cardiovascular and periodontal disease: comparative study. Clin Diagn Lab Immunol. 2002; 9(2):425-432. 82- Czerniuk MR, Górska R, Filipiak KJ, Opolski G. Inflammatory response to acute coronary syndrome in patients with coexistent periodontal disease. J Periodontol. 2004; 75(7):1020-1026. 83-Abou-Raya S, Naeem A, Abou-El KH, El BS.Coronary artery disease and periodontal disease: is there a link? Angiology. 2002; 53(2):141-148. 84- Aronow WS. C-reactive protein. Should it be considered a coronary risk factor? Geriatrics. 2003; 58(5):19-22,25. 85- Katz J, Chaushu G, Sharabi Y. On the association between hypercholesterolemia, cardiovascular disease and severe periodontal disease. J Clin Periodontol. 2001; 28(9):865-868. 86- Johnson C, Patel G, Messieha Z. The relationship between coronary artery disease and periodontal disease. Dent Today. 2003; 22(2):100-105. 87- Beck JD, Slade G, Offenbacher S. Oral disease, cardiovascular disease and systemic inflammation. Periodontol 2000. 2000; 23:110-120. 88- Dye BA, Choudhary K, Shea S, Papapanou PN. Serum antibodies to periodontal pathogens and markers of systemic inflammation. J Clin Periodontol. 2005; 32(12):1189-1199. 89- Blum A, Front E, Peleg A. Periodontal care may improve systemic inflammation. Clin Invest Med. 2007; 30(3):E114-117. 90- Doğan N, Orhan K, Günaydin Y, Köymen R, Okçu K, Uçok O. Unerupted mandibular third molars: symptoms, associated pathologies, and indications for removal in a Turkish population. Quintessence Int. 2007; 38(8):e497-505. 91- Al-Khateeb TH, Bataineh AB. Pathology associated with impacted mandibular third molars in a group of Jordanians. J Oral Maxillofac Surg. 2006; 64(11):1598-1602. 92- Mehra P, Castro V, Freitas RZ, Wolford LM. Complications of the mandibular sagittal split ramus osteotomy associated with the presence or absence of third molars. J Oral Maxillofac Surg. 2001 Aug; 59(8):854-8; discussion 859. 93-Marzola C, Pagliosa C. Impacted lower third molars surgery- a contest to the health. Rev. Bras. Cirurgia Buco-Maxilo-Facial. 2011; 10(2):29-42. 94- Fränzel W, Gerlach R, Hein HJ, Schaller HG. Effect of tumor therapeutic irradiation on the mechanical properties of teeth tissue. Z Med Phys. 2006; 16(2):148-154. 95- Zadik Y, Levin L. Decision Making of Israeli, East European, and South American Dental School Graduates in Third Molar Surgery: Is There a Difference? J Oral Maxillofac Surg2007: 65:658-662. 96- Guidance on the extraction of wisdom teeth . National Institute for Clinical Excellence (NICE); 2000. 12 p. (Technology appraisal guidance no.1). http://www.nice.org.uk/nicemedia/live/11385/31993/31993.pdf 97- Prophylactic Removal of Wisdom Teeth: A Review of the Clinical Benefit and Guidelines.Canadian Agency For Drygs And Technologies in Health. Healt Technologiy Assessment HTA. Agost 2010 http://cadth.ca/media/pdf/l0202_removal_wisdom_teeth_htis_2.pdf 98- Mettes DTG, Nienhuijs MMEL, van der Sanden WJM, Verdonschot EH, Plasschaert A. Interventions for treating asymptomatic impacted wisdom teeth in adolescents and adults. Cochrane Database of Systematic Reviews 2005, Issue 2. Art. No.: CD003879. 99- Friedman JW. The Prophylactic Extraction of Third Molars: A Public Health Hazard. American Journal of Public Health 2007; 97( 9):1554-1559. 100-Jongh A, Olff M, Hoolwerff H, Aartman I, Broekman B, Lindauer R, Boer F. Anxiety and post-traumatic stress symptoms following wisdom tooth removal. Behaviour Research and Therapy 2008;46: 1305-1310. 101-Garip H, Abali O, Goker K, Gokturk U, Garip Y. Anxiety and extraction of third molars in Turkish patients. Br J Oral Maxillofac Surg. 2004; 42(6):551-554. 102-Majid OW, Mahmood WK. Effect of submucosal and intramuscular dexamethasone on postoperative sequelae after third molar surgery: comparative study. Br J Oral Maxillofac Surg. 2011;49(8):647-652. 103- Barbosa NL, Thomé AC, Costa C, Oliveira J, Scariot R. Factors associated with complications of removal of third molars: A transversal study. Med Oral Patol Oral Cir Bucal. 2011; 16 (3):e376-80. 104-Gbotolorun OM, Olojede AC, Arotiba GT, Ladeinde AL, Akinwande JA, Bamgbose BO.Impacted mandibular third molars: presentation and postoperative complications at the Lagos University Teaching Hospital.Nig Q J Hosp Med. 2007; 17(1):26-29. 105- Clauser B, Barone R, Briccoli L, Baleani A. Complications in surgical removal of mandibular third molars. Minerva Stomatol. 2009; 58(7-8):359-366. 106- Akadiri OA, Okoje VN, Arotiba JT. Identification of risk factors for short-term morbidity in third molar surgery. Odontostomatol Trop. 2008; 31(124):5-10. 107- Almendros N, Berini L, Gay C. Influence of lower third molar position on the incidence of preoperative complications. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 ; 102(6):725-732. 108- Erdogan Ö,Tatlı U, Üstün Y, Damlar I. Influence of two different flap designs on the sequelae of mandibular third molar surgery. Oral Maxillofac Surg (2011) 15:147-152 109-Mead SV. Incidence of impacted teeth. Int. Orthodont. oral Surg. Radiol., 1930;(16):885-890. 110- Cogeswell, WW. Variations in normal anatomic struture. J. Oral Sint. Ass. 1933;(20);2:1423-1427. 111-Avellanal, C. D. Cirugía odontomaxilar. Buenos Aires: Ed. Ediar, 1946. 112- Ward TG. The split bone technique for removal of lower third molars. Brit. dent. J, 1956;201; 297-304. 113- Maurel, G. Clinica y Cirugía maxilo-facial. Buenos Aires: Ed. Alfa, 1959. 114- Kruger, G. O. Management of impactions. Dent. Clin. N. Amer.1959; 707-722. 115- Ries Centeno GA. El tercer molar inferior retenido. Buenos Aires: Ed. El Ateneo, 1960. 116- Szmyd L. Impacted teeth. Dent Clin North Am 1971;15:299-318. 110- Berwick WA. Alternative method of flap reflection. Br Dent J 1966;20;121(6):295-296. 117-Howe GL The management of impactedmandibular third molars. In: Minor oral surgery. 2. ed. cap III, p.41-71. Bristol, 1971. 118- Lotter R. Periodontal considerations in the extracion of retained wision teeth varyng technics. Chir. Dent. Fr., 1984; 252:(5);35-44. 119- Berzaghi, CM Curcio R. Incisão em M.Revista da Ass. Paulista de Odontologia, 1989;43(5):32-34 120-Stevão EL, Azoubel E. Técnica alternativa para remoção de terceiros molares submucosos e intra-ósseos da mandíbula, BCI .1998;5(2):15-19. 121- Incisions for third including lower molar. Silva F Cabral RJ, Felipe G, Machado E. International Journal Of Dentistry, Recife, 2006;1(1): 30-34. 122-Suarez M, Gutwald R, Reichman J, Otero X, Schmelzeisen R. Marginal flap versus paramarginal flap in impacted third molar surgery: A prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:403-408. 123-Nageshwar. Comma Incision for Impacted Mandibular Third Molars. J Oral Maxillofac Surg 2002;60:1506-1509. 124-Cetinkaya B, Sumer M, Tutkun F, Sandikci E, Misir F. Influence of different suturing techniques on periodontal health of the adjacent second molars after extraction of impacted mandibular third molars.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 125- Rosa AL, Carneiro MG, Lavrador MA, Novaes AB Jr. Influence of flap design on periodontal healing of second molars after extraction of impacted mandibular third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 93(4):404-407. 126- Karaca I, Şimşek S, Uğar D, Bozkaya S. Review of flap design influence on the health of the periodontium after mandibular third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:18-23. 127-Sanchis JM, Hernández S, Peñarrocha M. Flap repositioning versus conventional suturing in third molar surgery. Med Oral Patol Oral Cir Bucal. 2008;13(2):E138-42. 128- Kirk D, Liston P, Tong D, Love R. Influence of two different flap designs on incidence of pain, swelling, trismus, and alveolar osteitis in the week following third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:1-6. 129-Sandhu A, S. Sandhu S, Kaur T. Comparison of two different flap designs in thesurgical removal of bilateral impacted mandibular third molars. Int. J. Oral Maxillofac. Surg. 2010; 39: 1091-1096. 130-Arta SA, Kheyradin RP, Mesgarzadeh AH, r Hassanbaglu B. Comparison of the Influence of Two Flap Designs on Periodontal Healing after Surgical Extraction of Impacted Third Molars. J Dent Res Dent Clin Dent Prospects 2011; 5(1):1-4.
131-Martins L,. Lemes CH, Zardo M, Egg CM. Evaluation of periodontal healing on the distal of lower second molars, using two types of flap designs for removal of impacted third molars.Publ. UEPG Biol. Health Sci., Ponta Grossa, 2007;13 (3/4): 73-80.
132-Kırtıloğlu T, Bulut E, Sümer M, Cengiz I. Comparison of 2 Flap Designs in the Periodontal Healing of Second Molars After Fully Impacted Mandibular Third Molar Extractions. J Oral Maxillofac Surg 2007; 65:2206-2210. 133- Jakse N, Bankaoglu V, Wimmer G, Eskici A, Pertl C. Primary wound healing after lower third molar surgery: Evaluation of 2 different flap designs. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002; 93:7-12. 134- Pasqualini D, Cocero N, Castella A, Mela L, Bracco P. Primary and secondary closure of the surgical wound after removal of impacted mandibular third molars: a comparative study. Int. J. Oral Maxillofac. Surg. 2005; 34: 52-57. 135-Infante P. Post operative comparison of two flap designs in inferior third molar surgery. Rev Esp Cir Oral Maxilofac 2009;31(3):185-192.
136-Laissle G ,Aparicio P, Uribe F, Alcocer D. Post operative comparison of two flap designs in lower third molar surgery. Rev Esp Cir Oral Maxilofac 2009;31(3):185-192.
|
|
Publicado el: 30/12/2011 09:56:39 |