Información General Información General |
| Artículos |
| Notícias |
| Enlaces |
| Contactar |
| Buscar |
| Premio Nadal |
| Formación Continuada |
 |


Articulators: a historical review |
|
Publicado el: 11/01/2011 15:57:31  | |
| Alberto Forcén Báez, Ph. D., Juan F. Martínez- Lage Azorín, M.D., María-Teresa Ruiz Navas, Ph.D. Teaching Unit of Stomatologic Prostheses and Occlusion, University of Murcia Medical School, Hospital Morales Meseguer, 30008 Murcia, Spain.
Corresponding author: Alberto Forcén Báez. Calle Oscura, 20. 30170 Mula. Murcia. E-mail: aforcen@um.es ABSTRACT We review the current use and indications of dental articulators. We provide a review on the evolution of the ideas on occlusion and the different articulator devices developed by the diverse researchers on the subject. We also analyze mandibular dynamics and its implications in presently used articulators. KEY WORDS: Articulators. Gnatology. Dental Occlusion Acknowledgements We very much appreciate Raúl Melendreras Ruiz, odontologist of this Faculty, for the preparation of the art work. •1. INTRODUCTION The articulator is a mechanical device by means of which we can relate the models of the dental arc of the patients in order to realize diagnostic and therapeutic procedures outside of the mouth. Besides this, we can utilize the facial bows to transfer the same relation existing with the skull (with regard to the turn axis of the jaw and to a plane of reference) (1). The articulator is an essential device in order to work at a certain level, although some treatments can be carried out without articulator. These devices emerged from the necessity of being able to imitate the mandibular movements outside of the patient mouth. The mandibular movements depend on the governing factors of the dental occlusion (2), from which we may distinguish four: •· Articular factors •· Dental factors •· Arc factors •· Muscular factors The articular factors can only be modified when the surgery is utilized and they have to be adjusted in the articulators in order to restore the occlusion of the patient, once they have been acting on the dental and the arc factors.
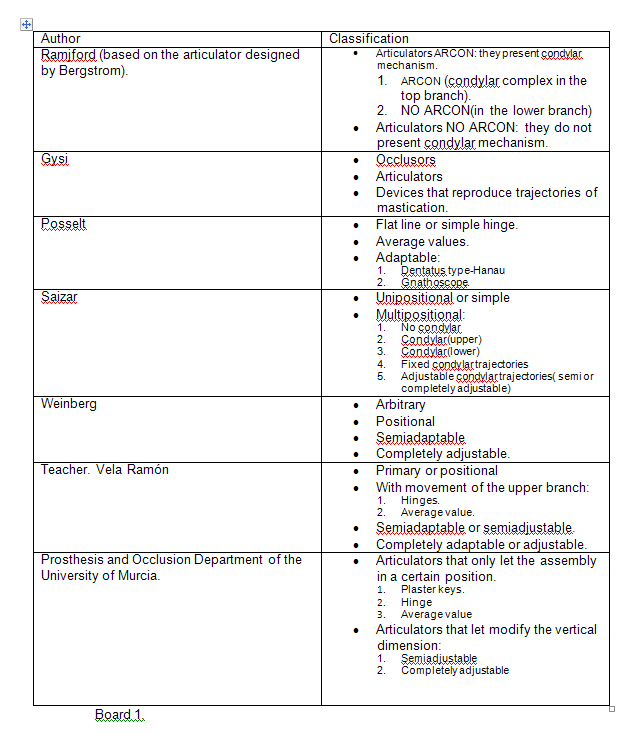
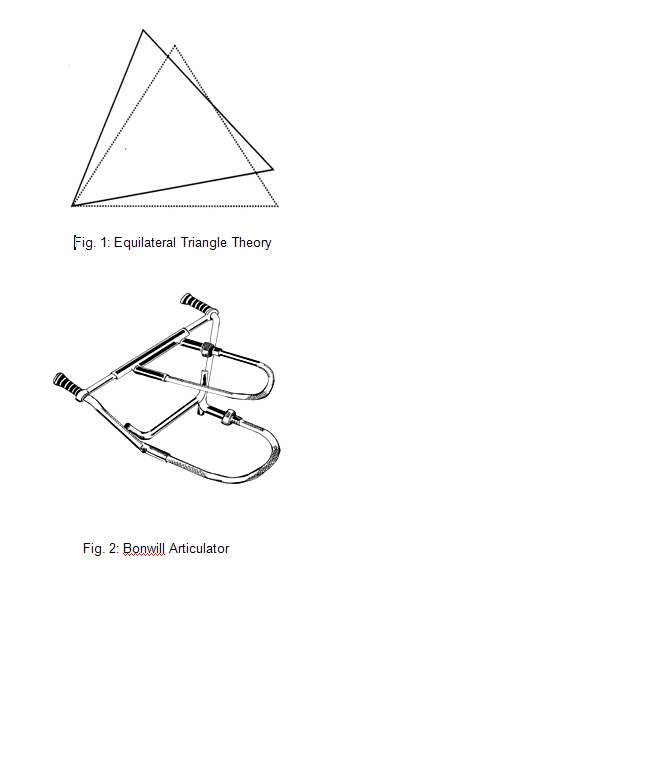
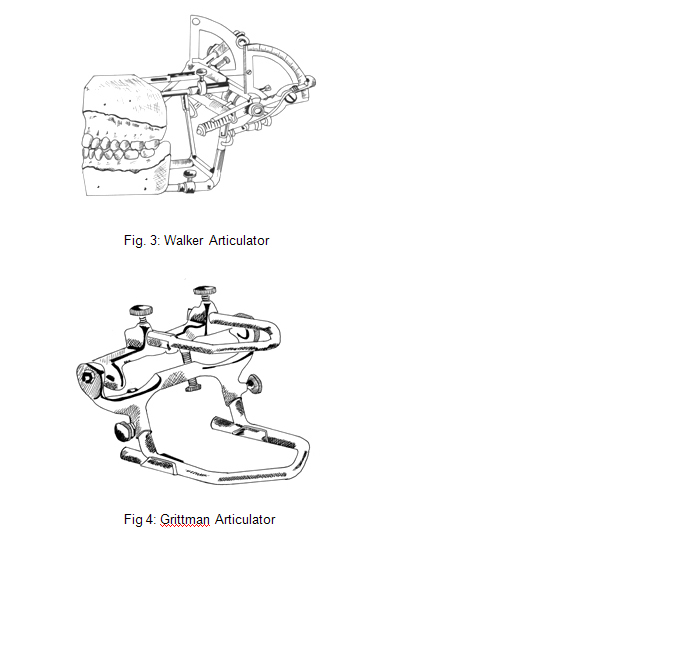
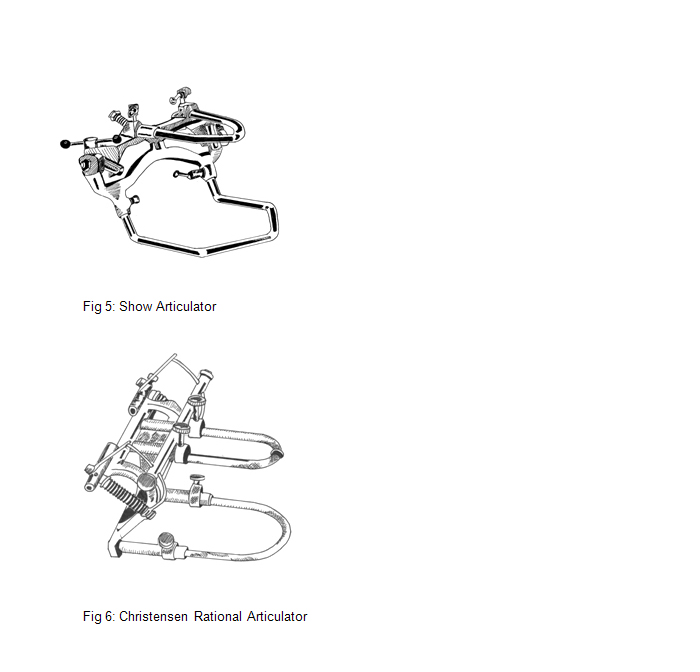
•2. PRECEDENTS The history of the articulators is recent relatively. The dental prostheses had only a cosmetic and phonetic function until the publication of the book "Le Chirurgien Dentiste" by Pierre Fauchard in 1728. Once the mentioned book was published, the prostheses started to be used to eat. We may divide the history of the articulators (3-7) into three stages characterized by their conceptual differences: 1st .- At a first moment, several tools were developed in order to antagonize models: plaster keys. Philip Pfaff (1713-1766) was said to be the first author who created a plaster key in order to antagonize and articulate the models in 1756. 2nd .- Subsequently, instruments with an opening and closure axis are designed: Articulators of hinge. Most of the authors consider Jean Baptiste Gariot as the responsible of the creation of the first articulator of hinge in 1805. The first articulator which provided a lateral movement was the one presented by Daniel T. Evens en 1840 it is thought that it was made by James Cameron. 3rd .- Finally, articulators that were based on scientific theories were created and they were called: Scientific articulators. This period started in 1858 approximately, when Bonwill enunciated the theory of the equilateral triangle, in which the intercondylar distance was of 10 cm and it forms an equilateral triangle with the interincisive point (figure 1). This geometric concept let him describe the condylar movements in the horizontal plane as pivotal movements around a condyle and the trajectory of the inferior incisives. Considering these data and the articulator described by Evens, Bonwill built an articulator to obtain a balanced occlusion (figure 2). This articulator had an even condylar trajectory, which never afforded complete balanced prostheses, until Walker (1896) transformed it aided by Bonwill's descriptions, adding adjustable condylar guides (figure 3). Walker carried out a complex extrabuccal mechanism to record the course of the condylar trajectory. In 1899, Grittman improved the concept of articulators, by increasing the space between the two arms, which always became parallel, which fixed the condilar trajectory on the upper arm (Fig. 4). Balkwill whose 1886 works were forgotten for a long time in a London's library, stated that (1) the mandible twists during the opening and closure movements around an axis that courses through both condoles, (2) the jaw moves in block during the lateral movement and (3)the condoles slip downward and forward during mandible protrusion. These proposals signaled a very important starting point for the study of the mandible dynamics, as until this moment, the existence of a mandible axis was unrecognized. In addition, Balkwill was the first to describe the condylar trajectory. This author designed an articulator called "Bite Frame" and used the instrument he had devised for measuring the condylar trajectory angle, known as face bow. Accordingly, we may consider Bonwill and Balkwill as the pioneers who gave birth to a body of knowledge in Occlusion science. In 1900, Snow developed his face bow, basing on Balkwill's work. We now may consider that the construction of the models in the articulator is more correct, as it relates the entire mandibular arc with the condyles, but it lacked a reference to a plane. The current face bows are based on their design. In addition, this researcher designed his own articulator (Fig. 5). In 1902, Carl Christensen affirmed that the trace of backward separation by intrabuccal wax during movements of the mandible protrusion allows calculating the condylar slope and devised the rational articulator (Fig. 6). Campion, in 1905, concluded that the models should be mounted on articulators, allowing that the rotation axis coincided with the opening and closure mandibular axis. He described the mandibular movement in two phases: 1. - the mandible turns around an axis that passes through both condyles. 2. - in a second moment, the axis rotation is supplemented by a forward and downward translation displacement. In 1907, Bennet described the in-block mandible movement towards the laterality side and observed that the no-working side condyle moves forwards, downwards and inwards, being the trajectory different when the condyle remains fixed or when the jaw moves in block towards the side of the laterality. In 1913 Alfred Gysi improved the theory of the cylinders started by Bonwill and Balkwill and he designs the articulator Simplex. He said that the alterations of the temporomandibular articulation should be studied with models assembled on articulator and individual records and then they should be reproduced in the mentioned articulator to proceed to the diagnosis and the adequate treatment. Besides, he introduced the inclination of the incissal guide and the gothic arc tracer. By means of graphic records and mathematical calculus he achieves the instant centres of rotation in the different mandibular movements. There are six cylinder axes which govern the mandibular dynamics. The intersection of the cylinders axis of the opening and closure movements and of the laterality movements is defined as the mandibular centre of rotation, which is situated in an anterior, inferior and lateral position to the intercondylar axis. It is a variable point in its location and, therefore, it is an instantaneous centre of rotation. The situation of this centre is justified, because it is the point or region that is less displaced in the mandibular movements. Besides, the vascular-nervous system which nourishes the mandible is joined to the bone approximately to this height (Spix spine). According to the theory of the cylinders the pure rotation is not considered, because the movement of openness and closure is not regarded as a whole. According to the works by Von Spee (which describes the compensation curve which has its name in 1896) and the theory of Bonwill, Monson created the sphere theory, in 1918, developing an articulator that has not got an intercondylar axis. He considered that the lower dental arc is displaced above the upper one in a pendular way and it describes a part of the sphere whose centre is located on crista galli apophysis and its turning circle would be 10, 4 cm. On the surface of this sphere the occlusal plane and both temporomandibular joints were also included. Villain also studied the sphere theory and he stated that the teeth were placed in the superior arc following a parabolic curve, converging its biggest axis towards an area situated three centimetres behind the nasion, which should be considered as the rotation centre in the mastication movements. Rudolph Hanau (1921-1922) registered sagittal and lateral inclinations with wax intraoral records and he developed an articulator which is still used nowadays: H by Hanau model. The inclination of the condylar slope may be adjusted in such model, but it is rectilinear. He also developed the Kinoscopy with a double condylar mechanism and proposed a formula to calculate the Bennett angle. Condylar trajectory Bennett angle= ........................+ 12 8 In 1926 B.B. Mc Collum founded the Gnatologic Society in Los Angeles with H. Stallard and C.E. Stuart and they are creating the bases of Gnatology which studies the movements of ATM in order to measure, reproduce and use them as determiners of the diagnostic and treatment of occlusion. Mc Collum and Stuart built an articulator the Gnatograph that could duplicate in a real way the mandibular relations and the condylar movements so that the teeth occlude in an ideal way. They developed the cinematic facial arc in order to locate the axis of rotation and the pantography in order to adjust the articulators. From the beginning they advocated the balanced occlusion for the subjects with teeth. They rejected this concept thirty years later and they adopted the canine disclusion from D'Amico. This school bases the creation of the rehabilitation on the discovery of the hinge axis, recording and the reproduction of the axis movements and the realization of the occlusion morphology with these determining factors. From 1955 to 1956 Stuart developed the articulator which has its name. It is an "arcon" articulator completely adjustable with its pantograph in order to adjust such pantograph. In 1958 the articulator Dentatus A.R.L. appeared and it was designed by Arne G. Lauritzen which is very similar to Hanau H2 and it has a slightly curved incissal shoot. It has a very small screw in order to measure the extent of the movements. Stuart designs in 1964 an articulator semiadjustable arcon type where the intercondylar distance can be adjusted in three pre-established positions and with condylar and plane guides by Bennet and a straight incissal shoot. The Denar house commercialized the Denar D.Y.A., in 1968 and it was designed by Niles Guichet. It is an adjustable articulator which can be adapted to plastic guides through a pneumatic pantograph in order to imitate the mandibular movements. Later, electronic pantographs are developed where the results are taken from the system printer and they are adapted to the articulator. •3. BASIS OF THE ARTICULATORS
The most of the mandible movements does not follow any geometric pattern. By means of the articulator, we try to imitate the following basic mandible movements:
1. Movement of opening and closure. 2. Movement of protrusion. 3. Movement of laterality.
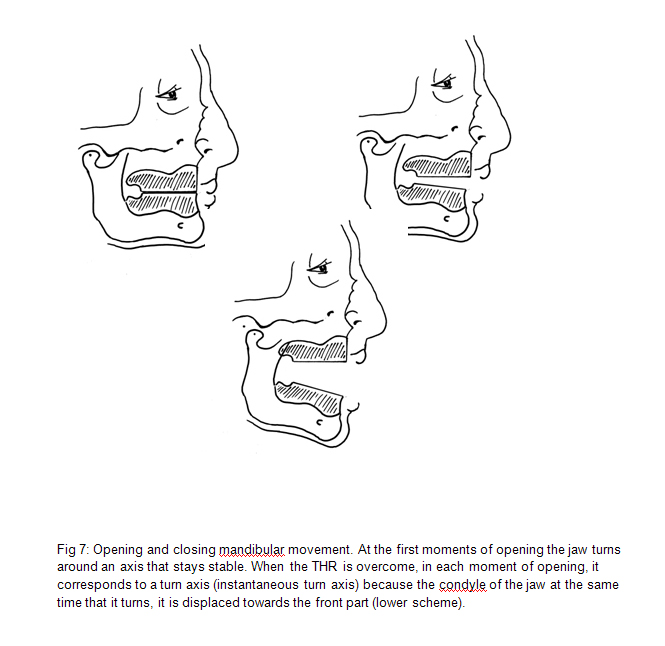
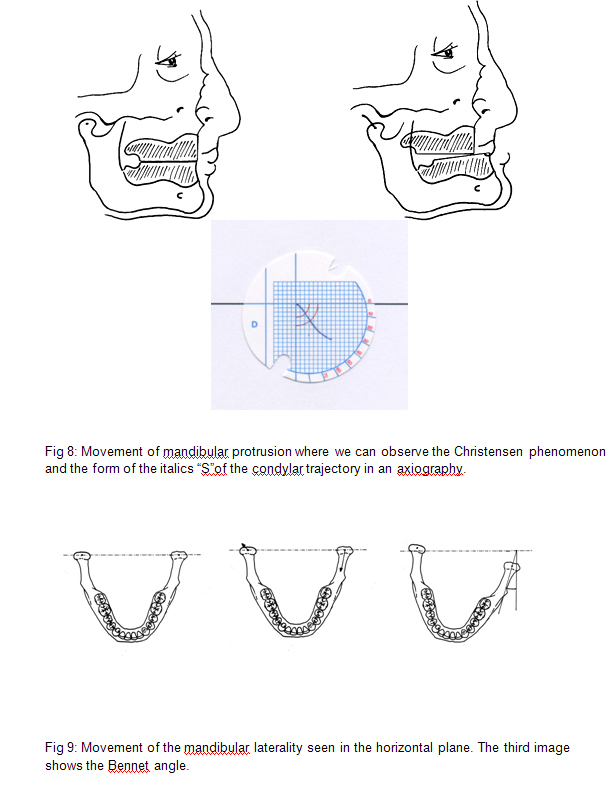
1. Movement of opening and closing It is the only movement which follows a geometric pattern. When the jaw is in centric relation, the first moments of opening, approximately 12º, (Terminal Hinge Relation or THR) are realized according to the terminal hinge axis (Terminal Hinge or TH). If this capacity is overcome, while it is spinning, the condyle suffers a displacement, which generates an instant rotation axis in each new mandible position that it is only determinable in a mathematical way. (Figure 7) The THR is reproducible in the articulators when the mechanical axis of the instrument coincides with virtual axis of the patient. This fact involves two events: •· The need to locate the rotation axis of the patient. The axis beepers are used and the projection of the axis is obtained on the skin. •· The need to transfer the superior jaw of the articulator in the same situation which has got according to this axis and a reference plane. For this reason, it is very important the use of facial bows. The movement of opening and closure is so important, because it is concerned with the modification of the vertical dimension, whose consequences we will study subsequently. 2. Movement of protrusion It is ruled by the condylar guide. When the mandible realizes a movement of protrusion, this guide generates a trajectory, which has got the shape of an extended "S" in italics, because any point located in the mandibular condyle(where it is included the rotation axis) is displaced downwards and forwards (figure 8). For this reason, when the mandible realizes a movement of protrusion, a separation of the back segments of the dental arc is produced. This phenomenon was described by Christensen according to the complete prosthesis and it is one of the methods used in order to adjust the condylar slope of the semiadjustable articulators. The pantography is utilized in order to determine the condylar trajectory. It is a technique used to draw the real trajectory of the jaw. Subsequently, the same trajectory of the articulator is tried to be reproduced. Summing up, the semiadjustable articulators let the adjustment of the condylar slope, which is straight generally (it is curve for some articulators, what it does not represent any disadvantage, because it is not the real one for the patient). The articulators which are fully adjustable let the adjustment of the condylar trajectory, being the movements of protrusion and the movements of the patient the same. 3. Movement of laterality It is the most difficult movement to conceive and to reproduce concerning the articulators (Posselt, 1973), because it is the most complex movement we may find (8). The factors that rule the laterality movements are: I. Trajectory of the nonworking side: The condyle of the nonworking side is displaced downwards, forwards and inside and it generates the trajectory of the nonworking side.
II. Trajectory of the working side: The condyle of the working- side is lateralized and is liberated from the articular cavity, so that the jaw could turn. From this point, the condyle can be moved in any direction and if it was represented in the space, it would create a cone of condylar apex in whose base all the possibilities of movement were possible. It is normally displaced outside, upwards and backwards and it represents the movement of Bennet that takes place in all the jaw.
III. Intercondylar distance or length of the back axis. It is the factor which has less significance in the movements of laterality (figure 9), because the variation in the width of the face among the different patients is small (Dawson, 1991) and the difference in the route of the cusps is not really important. We may say that when a movement of laterality is realized, the jaw needs to move in block towards the side of the laterality (movement of Bennet), in order to allow the rotation of the condyle (De Pietro 1972). For this reason, the movement of rotation is not pure. In the trajectory of the working side, the width of the movement is small, but it gives complexity to the movement of laterality. The semi-adjustable articulators do not normally allow fixing the direction of the Bennet movement, which will always be realized in the prolongation of the intercondylar axis in repose (position of centric relation). However, the shift angle lets the fixing of Bennet movement direction. Besides this, there is an angle which is formed between the condyle trajectory in a protrusion movement and a laterality movement. This angle is called the Fisher curve angle and it has not got any clinic importance, because it cannot be adjusted in the habitual articulators. Finally, we may point out that there are different procedures to adjust the Bennett angle, such as the use of standard figures, plastic records of the laterality movements or the utilization of formula which are dependent on the condylar slope, the axiography and the pantography. 4. CLASSIFICATION OF THE ARTICULATORS There are several classifications, because each author has realized a classification according to his/her point of view about occlusion (see table 1). We point out our categorization, as it is useful from a clinical point of view and it is divided into: •· Articulators that only let its setting on a certain setting. •· Articulators that allow modifying the vertical dimension. The plaster keys do not have any opening and closure axis, so the superior element is independent from the inferior one. They have the same function that the following two articulators, but they are more uncomfortable to use. The hinges have got a rotation axis, but they do not coincide with the opening and closure axis of the patient, so the axis only provides comfort in the realization of the prosthetic work, because the elements of the articulator are not separated, The articulators of the average value present the condylar and incisal guides adjusted to certain standard values, even some of these articulators have also adjusted the Bennett angle. As they are standard values, the movements that reproduce do not coincide with the movements of the patient. It is possible to make an exception because some of them can admit a facial bow and therefore they can do cranium-jaw transference in the same relation that it keeps with the patient with regard to the rotation axis (9). In this way, the movement of opening and closure in the THR bow would be coincident with the movement of the patient, but only when we have located the real rotation axis. If we determine a standard axis, the movement will be approximate. The rest of the movements are not coincident with the movements of the patient and with any position because the values are standard. The coincidence will be rare. It is not reasonable to realize the manoeuvre of localization of the hinge axis and after that to work with the articulators of fixed guides. The semiadjustable articulators only reproduce exactly the movement of opening and closure and some positions that we will use later for the adjustment of the instrument. So, when we register a protrusive position of for example 5 mm, for the adjustment of the angle of the condylar slope, the position of the models will coincide with the movements of the patient when we put the articulator in a distance of 5 mm. In other positions, there will not be any coincidence, but it will be approximate. In the same way, registers of laterality may be used to adjust the Bennett angle. For this reason, the movement realized by the articulator from the centric relation to the position of 5 mm, might not be able to coincide with the patient movement, although the articulator has curved condylar guides. The adjustable articulators reproduce similar movements to the patient´s ones such as the movement of opening and closure in hinge terminal axis. The pantograph is used to make the adjustments. This characteristic will help us be more precise in the elaboration of prosthesis and it will not be necessary to overextend when an incisal or canine guide is realized in order to get disclusion. 5. CLINICAL CONSIDERATIONS
A) According to the articulators: On the one hand, the classification realized lets us choose the most appropriate articulator concerned with what we want to achieve with the treatment.
If we use a hinge or an articulator of average values, we will be able to work with the maximal intercuspidation position, or in centric relation (if it has to do with a complete prosthesis made with a specific technique), but there will not be any possibility to modify the vertical dimension or to check the centric relation validity. If the articulator lets excursive movements, they will be very different to the patient's ones, in such a way as isolated teeth, small bridges, and not very important prosthesis could be replaced when the patient does not present any symptom or sign of occlusal illness whose treatment would be a different one. On the other hand, most of the prosthetic treatments need an assembly of the prostheses at the maximal intercuspidation and the doubt which emerges has to do with the relation of the models' assembly. There are two possibilities: 1. Assembly at the maximal intercuspidation. If we make this assembly in the semiadjustable articulator, the movements of the articulator do not correspond to the movements of the patient and to the movements of closure and opening. We think that for this assembly, it is not necessary the use of a semiadjustable articulator. 2. Assembly in centric relation and subsequent work at the maximal intercuspidation. In this case the transference is adequate according to the turn axis and a reference plane, but the movements are not the same to the patients' ones (if we use a semiadjustable articulator) and they are the same with some positions. The advantage of this method is that it lets study the terminal retrusive trajectory in order not to leave any interference in it and in the trajectory of the working side. The easiest situation is the one where we want to realize a study in occlusion or rehabilitation. We will proceed to locate the turn axis and with the help of an axis-orbital facial arc, the cranial maxilar transference is made in at least a semiadjustable articulator. B) According to the facial arcs:
The cranial maxilar transference may be realized according to an arbitrary axis or the real turn axis. We think that the different facial arcs may behave in two ways depending on where the posterior element is applied, independently of how they are built mechanically. In order to transfer the real turn axis, we will need to locate the axis in the patient (locators such as Almore's and Stuart's locators) and to transfer the real turn axis through the facial arc. (10) If the posterior element, which is located previously through a locator device, is applied in the real turn axis, we will find an axis-orbital facial arc. If the mentioned arc is situated in a standard reference, for instance in a distance of 11mm in front of the tragus in a line that binds this and the eye's commissure, then we will find with a standard reference, being this craneomaxilar transference similar to the one which we had made with a facial arc of intaauricular olives. In addition to this, we may indicate that the existence of the turn axis provides us with a wide variety of advantageous characteristics: •· It facilitates the assembly of models as it is used as a subsequent reference. •· It lets the modification of the vertical dimension. •· It makes possible the validity of the record of the centric relation: two records of the centric relation will coincide if we are situated in the closure arc. •· It will not be necessary to make adjustments in the mouth (Kornfeld, 1972) if the prosthesis has been adjusted in the articulator where the turn axis has been transferred. This is what we know as reassembly and occlusal adjustment of the prosthesis. It is not always necessary to use an anterior reference of the facial arcs. We will use it in the following cases: 1. When the inclination angle of the condylar trajectory is adjusted through axiography. 2. When we work with the adjusted articulator at a certain average for example 40º sexagesimal. 3. When we use values got in previous explorations for the realization of a prosthetic work and in the realization of rehabilitation. 4. When we wish to keep the value of the inclination angle of the condylar trajectory in the medical history of the patient, determined through intrabuccal registers, in order to use it in subsequent situations. 5. When facial arcs of olives are used and the preceding part cannot be modified, because the axis does not coincide with the subsequent reference of the arc and the position of the axis and the occlusal plane change.
Nevertheless, in most of the cases where the assembly of models in an articulator is realized to make a study of occlusion or to make a certain prosthetic treatment, it is not necessary the use of the precedent element of the facial arc. In this case, the adjustment of the angle of the condylar slope is realized in the articulator through wax intrabuccal recordings and the only interesting aspect is that the disclusion produced in the articulator may be similar to the patient's one in a protrusive position. Finally, when facial axis-orbital arcs are utilized such as Almore's one, it is necessary to use articulators which have an extension of the turn axis, because the articulator has to find the facial arc otherwise we could run the risk of modifying the skull-maxilar transference.
6. CONCLUSIONS We may consider that it is enough to realize an assembly at the maximal intercuspidation to do most of the prosthetic works by using a hinge or an articulator of fixed guides, except for the case of occlusal problems (11). In those situations where we have to realize a modification of the intermaxilar relations (occlusal rehabilitation) (12, 13, 14) or when there is not a relation at the maximal intercuspidation, we will have to locate the turn axis and to make an assembly of models in a semiadjustable or an adjustable articulator. An example would be a toothless patient (unimaxilar or bimaxilar) who has been treated with implants. Finally, we regard the huge development produced in the new technologies as an important aspect for the occlusion studies, because they make the mentioned studies easier, more standardized and reliable and they let reduce the human mistake. Summing up, the study of the development of the articulators through history makes us think about the small advance in the diagnostic and therapeutic field in stomatologic prosthesis. 7. BIBLIOGRAPHY
•1. ASH MA, RAMFJORD SP. Oclusión funcional. México: Interamericana, 1984. •2. FORCÉN BÁEZ A, RUIZ NAVASMT, ROYO-VILLANOVA PÉREZ ML.Dinámica mandibular. Factores rectores de la oclusión dentaria. Revista Europea de Odonto-Estomatología 2001; 13(2):73-78. •3. DORIER, M. Encyclopédie médico-chirurgicale, Stomatologie. París. Tomo VII, 1961. •4. GONZÁLEZ IGLESIAS J. Historia Ilustrada de la Prótesis dental (III). Gaceta Dental. 1997; 77 abril 22-30. •5. GONZÁLEZ IGLESIAS J, ROMERO MAROTO M. Tratado de Odontología. Tomo I. Sección VIII. Historia de la odontología. Capítulos 1 al 10. Madrid: Smithkline Beecham, S.A., 1998. •6. GONZÁLEZ IGLESIAS J. Historia Ilustrada de la Prótesis dental (I). Gaceta Dental. 1997; 75 de febrero 36-44 •7. GONZÁLEZ IGLESIAS J. Historia ilustrada de la Prótesis dental (II). Gaceta Dental. 1997; 76 marzo, 16-24. •8. FORCÉN BAEZ A, RUIZ NAVAS MT, RAMOS CASTILLO MR, ROYO-VILLANOVA PÉREZ ML. Estudio de las posiciones de lateralidad mandibular en un articulador semiajustable, Revista Europea de Odonto-Estomatología. 1997, IX (I): 23-28. •9. FORCÉN BAEZ A, RUIZ NAVAS MT, ROYO-VILLANOVA PÉREZ ML. Transferencia craneomaxilar. Comparación de dos tipos de arcos faciales. Revista Europea de Odonto-Estomatología 1998; X: 39-42. •10. FORCÉN BAEZ A, RUIZ NAVAS MT, ROYO-VILLANOVA PÉREZ ML. Arcos faciales. Nueva clasificación. Revista Europea de Odonto-Estomatología 1998; 10 (2): 67-70. •11. DAWSON PE. Evaluación, diagnóstico y tratamiento de los problemas oclusales. Barcelona: Salvat, 1991. •12. KORNFELD M. Rehabilitación bucal. Procedimientos clínicos y de laboratorio. Buenos Aires: Ed.Mundi, 1972. •13. POSSELT U. Fisiología de la oclusión y rehabilitación. Barcelona: Editorial Jims, 1973. •14. CAMPOS A. Rehabilitación oral y oclusal. Madrid: Harcourt, 2000.
|
|
Publicado el: 11/01/2011 15:57:31 |